DO YOU KNOW WHAT A DEFENSIBLE LEGACY CER ACTUALLY LOOKS LIKE?
See the evidence, the reasoning, and the CER text; annotated for what a reviewer accepts and why.
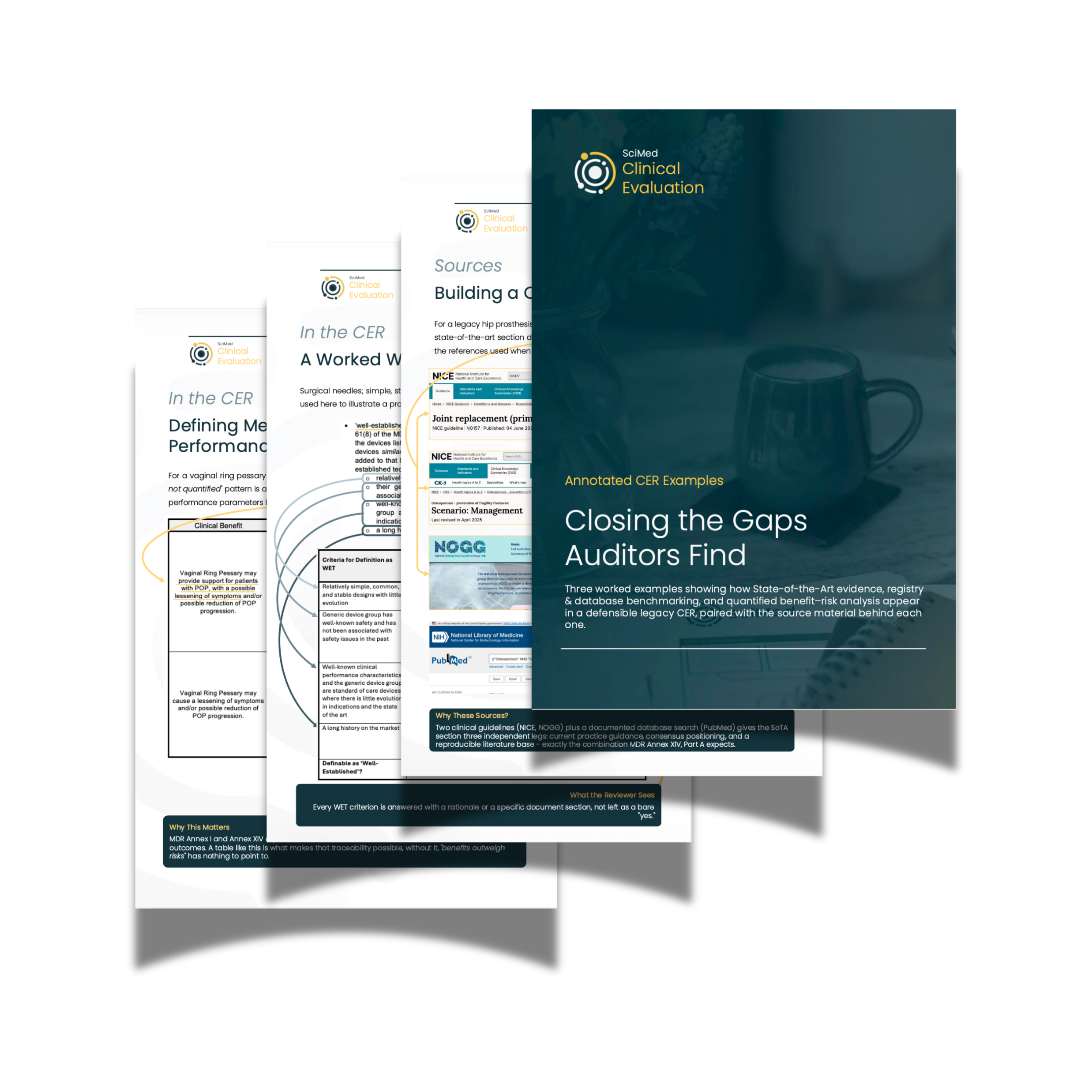
Three worked examples showing how State-of-the-Art evidence, registry benchmarking, and quantified benefit–risk analysis appear in a legacy CER that holds up under MDR scrutiny.
Covers the three patterns auditors raise most often on legacy devices
Source material and CER text shown side-by-side
Annotated for what makes each section reviewer-ready
Most Legacy CER Gaps Aren't Obvious Until a Reviewer Points Them Out
The gap is usually in the reasoning, not the references.
Teams working on legacy device CERs under MDR generally know the problems:
Frozen SotA,
A WET rationale that asserts rather than evidences, or
Benefit–risk conclusions with nothing behind them.
The challenge is knowing what the corrected version looks like; Guidance documents describe what a CER should contain. They don't show you what it looks like when the evidence and the conclusion are connected in a way a reviewer can follow and test.
The result is CERs that are complete on paper but vulnerable under scrutiny. A SoTA that names its sources but doesn't anchor them to current guidelines. A WET claim that lists the MDCG 2020-6 criteria but answers each with a bare "yes." A benefit–risk section that reaches a conclusion without first defining the measurable parameters it would need to demonstrate.
Finding those gaps before review requires knowing what the gap-free version looks like. That's what this resource shows.
Three Worked Examples, Built Around the Gaps Auditors Actually Raise
Each example covers one of the three patterns legacy device CERs most commonly fail on:
Identify what a frozen SotA section looks like, and see how to correct it - anchoring to current guidelines and a dated, reproducible search methodology.
See a WET rationale evidenced criterion-by-criterion against the requirements of MDCG 2020-6, with an explicit statement of the conformity route it supports.
Read a benefit-risk section that defines measurable parameters before it draws conclusions, and expresses risk using the same incidence-rate logic as the benefit claims.
Each pattern is presented across several pages. The source evidence page shows the guidelines, registries, and databases a reviewer would expect to see represented, and what each one is being used to establish. The CER excerpt page shows how that evidence appears in the clinical evaluation, with annotations explaining why the reasoning holds.
The examples use three representative legacy devices, a hip prosthesis, surgical needles, and a vaginal ring pessary - chosen because each illustrates a different evidence challenge: an established device with decades of registry data, a simple device that may qualify as Well-Established Technology, and one where benefit and risk both need to be expressed in measurable terms.
This isn't a template. The annotations explain why each section works, not just what it contains.
Who This is For?
This guide is written for the people working on legacy device CERs under MDR.
If you are a Regulatory Affairs Manager updating a CER that was written under the MDD, a QA/RA Director assessing whether your current documentation would survive notified body scrutiny, or a consultant working through common patterns, this resource gives you a concrete reference point.
It's particularly useful if you know what needs to change in your legacy CER but aren't sure what the corrected version should look like, or if you want to check your own reasoning against examples built to meet current reviewer expectations.
A Citation Isn't the Same as a Justification
Most CER sections that draw auditor comment aren't missing references. They're missing the connection between the reference and the conclusion.
The SotA names NICE guidelines but doesn't state what they establish about current standard of care. The WET rationale lists the MDCG 2020-6 criteria but answers each one with "yes." The benefit–risk section reaches a conclusion without defining the measurable parameters it would need to demonstrate.
Each example in this guide makes the logic visible, so you can apply the same reasoning to your own documentation.
“The difference between a citation and a reviewer-ready justification is usually in the framing, not the reference list.”
- Dr Alastair Selby
Seen These Patterns in Your Own CER?
Many manufacturers who work through examples like these recognise the same gaps in their own documentation. Knowing what the gap looks like is a starting point, but understanding what it means for your specific device, your evidence base, and your current submission timeline is a different question.
SciMed provides targeted Clinical Evaluation Gap Analysis for legacy devices under MDR. We review your current documentation, identify the sections most likely to attract scrutiny, and give your team a clear, prioritised view of where your evidence position needs to be strengthened.
Fixed fee. Written diagnostic in five working days. No scoping call required if you're ready to proceed.